![]() Please specify the quantity of product(s).
Please specify the quantity of product(s).




Kessler Foundation Prism Adaptation Treatment (KF-PAT) for Spatial Neglect
Kessler Foundation Prism Adaptation Therapy - A complete course of treatment for spatial neglect, a common complication of stroke that hinders recovery. Restores neural networks involved with spatial perception to achieve lasting results that enhance recovery in multiple domains.
| Item | Product | Price | QTY |
|---|---|---|---|
| 31100 | Kessler Foundation Prism Adaptation Treatment (KF-PAT) Kit | $4,095.00 | |
| 31100M | KF-PAT Manual | $60.00 | |
| 31100R | KF-Pat Right-Based Prism Lenses | $550.00 | |
| 31100L | KF-PAT Left-Based Prism Lenses | $550.00 | |
| 31100C | KF-PAT Visual Field Occluder | $160.00 | |
| 31100S | KF-PAT Visual Field Occluder Stand | $525.00 | |
| 31100P | KF-PAT Position Board | $897.00 | |
| 31100U | KF-PAT Ruler Board | $275.00 | |
| 31100V | KF-PAT Visual-Proprioceptive Task (VPT) Box | $825.00 | |
| 31100G | KF-PAT Opaque Cape | $120.00 | |
| 31100K | KF-PAT Kit Binding Strap | $50.00 | |
| 31100B | KF-PAT Carrying Bag | $275.00 | |
| 31100E | KF-PAT Eye Mask, Pk/30 | $35.00 | |
| 31100F | Pen - Dry Erase, Red | $11.00 | |
| 31100T | KF-PAT Laminated Printed Stimuli Sheets, Pk/60 | $50.00 | |
| 31100N | Neck Wraps, Pk/50 | $33.00 |
Kessler Foundation Prism Adaptation Treatment (KF-PAT)
Peii Chen, PhD & Kimberly Hreha, EdD, OTR/L
- Patented portable system
- Complete system with manual to administer the entire course of treatment
- Ongoing clinical and technical support
- Extensive research support
Kessler Foundation Prism Adaptation Treatment (KF-PAT) is a complete system to administer prism adaptation treatment for the treatment of spatial neglect. Prism adaptation uses prism goggles (goggles with lenses tilted either to the right or left) to effect a visuomotor phenomenon (prism adaptation), which improves spatial neglect. Researchers at Kessler Foundation who developed this device and treatment protocol have conducted extensive research involving federally funded clinical trials that have resulted in numerous peer-reviewed journal articles (see Details Tab for references). Prism adaptation treatment has been recommended as a frontline treatment for spatial neglect by the American Heart/Stroke Association, the Canadian Stroke Association, and in many meta-analyses and systematic reviews.
Spatial neglect is a syndrome caused by damaged neural networks critical for attention and related functions in the brain. Because attention, especially spatial attention, is essential for a wide variety of functions, spatial neglect affects many perceptual, cognitive, and motor functions. Deficits caused by spatial neglect disrupt basic self-care activities (e.g., dressing, grooming), impair postural balance, interfere with reading ability, and impede navigation.
 >
>
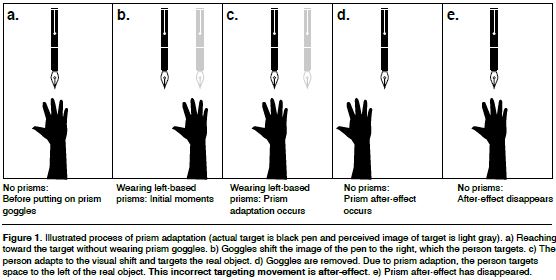
The KF-PAT treatment is typically administered over 10 sessions of approximately 20 minutes each. Patients wear goggles that shift their vision slightly horizontally while reaching for targets presented by the therapist. Visual feedback regarding the missed target is “sent” to the motor system, which corrects the subsequent attempts to reach towards the target. This process is then repeated with the goggles removed. Because the patient's motor system had adapted to the image shifted from the actual target by the goggles, the patient is again off-target when reaching for the target, but then adapts to this distortion and is able to again accurately reach to the target.
This entire process of adaptation helps bring attention and awareness to the neglected side of space and improves symptoms of spatial neglect. The benefits of this treatment compared to others is that:
- Improvements occur automatically. Patients do not have to learn skills, read, remember information, or perform other actions that may be difficult for those with symptoms of stroke.
- Most patients can participate. The movements necessary are minimal, and because the KF-PAT has a patented portable design, the treatment can even be brought to patients for whom travel would be difficult.
- Effects are sustained. Treatment occurs at a fundamental neurological level. Thus, changes that occur do not require deliberate effort or are the result of skills that may be forgotten or neglected.
The KF-PAT administration protocol has two built-in assessments of pointing performance, both administered before and after prism adaptation, to help you detect and measure prism after-effects in two different ways. The two assessments are Proprioceptive Pointing and Visual-Proprioceptive Pointing:
Proprioceptive Pointing
- During the Proprioceptive Pointing task, patients will point straight ahead while blindfolded. You will assess the patient’s deviation from their midline. This task assesses the patient’s innate sense of proprioception without visual cues. That is, they rely on their proprioception to make the movement.
Visual-Proprioceptive Pointing
- During these tasks, patients will point at a visual target (hence “visual” in the name of this task), i.e., a pen held up by the therapist, while they are blocked from seeing their own arm, hand, or fingers when making the reaching and pointing movement (hence “proprioceptive” in the name of the task). You will assess the deviation of patient’s pointing, which indicates the (mis)alignment between the patient’s visual and motor systems.
After-Effect - As stated, both pointing tasks are administered before and after prism adaptation, thus creating four assessment conditions. Data is collected by the therapist during those tasks, and the change in performance from before to after treatment is calculated and recorded in included reproducible record and summary forms.
Therapist Qualifications:
You should have advanced training and/or an educational degree with advanced coursework in neuro-rehabilitation of individuals with stroke or brain injury, or work under the license of someone with these credentials. Qualifications that typically fulfill these qualification requirements are: occupational therapists (OTs), physical therapists, aka physiotherapists (PTs), speech and language pathologists (SLPs), clinical psychologists, neuropsychologists, neurologists, and physiatrists.
The KF-PAT manual is designed to guide everyone through the steps of training and learning to administer the KF-PAT so that they can administer an entire course of KF-PAT treatment. Ongoing clinical and technical support is provided. Additional training may be acquired. Please contact us for details and options.
The KF-PAT Kit (31100) contains all the equipment listed below. All equipment is necessary to administer the KF-PAT treatment protocol.
KF-PAT Components
|
Right-Based Prism Lenses |
|
|
|
|
|
Left-Based Prism Lenses |
|
|
|
|
|
Position Board |
|
|
|
|
|
Ruler Board |
|
|
|
|
|
Visual‐proprioceptive task (VPT) Box |
|
|
|
|
|
Visual Field Occluder |
|
|
|
|
|
Visual Field Occluder Stand |
|
|
|
|
|
Opaque Apron |
|
|
|
|
|
Kit Binding Strap |
|
|
|
|
|
Carrying Bag |
` |
|
|
|
|
Eye Mask (pk/30) |
|
|
|
|
|
Pen |
|
|
|
|
|
Laminated Printed Stimuli Sheets |
|
|
|
|
|
Neck Wraps (pk/50) |
|
|
|
|
|
KF-PAT Manual |
 |














Treat Spatial Neglect From Stroke
Improve Functional Recovery After Stroke
Spatial Neglect
- Affects 30-50% of stroke patients
- Majority do not realize it
- Debilitating- Interferes with mobility, self-care, navigation, reading, employment, safety
- Requires treatment for improvement
- Improving spatial attention and spatial awareness leads to improvement in other domains
Missing Critical Information Can Have Devastating Consequences
Prism Adaptation Treatment
- Treats neural networks- Sustained improvement
- Evidence-based- Recommended by medical associations
- Easy for patients to participate
- Improvements seen within 10 sessions of 20 minutes
KF-PAT Supplementary Information/Material:
- Sample from the KF-PAT Manual
- Prism After-Effect Sheet Downloadable
- Nausea Profile Form Downloadable
Demonstration of the KF-PAT System:
- To see a brief demonstration video, click here: KF-PAT Demonstration Video
Additional Information:
- For more information on KF-PAT, click here: Understanding Prism Adaptation: A Rehabilitation Technique for Spatial Neglect
- For more information on spatial neglect, click here: Understanding Spatial Neglect
- Check out this Real Life Science podcast where spatial neglect and KF-PAT are discussed: Shifting Perspectives: Prism Adaptation and Stroke Recovery Real-Life Science Audio Summary
References
Suggested APA 7th ed. Reference for KF-PAT:
Chen, P. & Hreha, K. (2020). Kessler Foundation Prism Adaptation Treatment 2020 manual, Stoelting.
Complete References from Manual
Relevant Publication
- Hreha et al 2022.pdf
- The Implementation Process of Two Evidence-Based Protocols: A Spatial Neglect Network Initiative, Frontiers in Health Services
- Chen et al 2022 PAT Dosage Matters.pdf
- Impacts of Prism Adaptation Treatment on Spatial Neglect and Rehabilitation Outcome: Dosage Matters, American Society of Neurorehabilitation
Selected References of Prism Adaptation Efficacy
- Chen, P., Hreha, K., MacPhee, C., Salter, A., & Eskes, G. A. (2025). Does prism adaptation treatment reduce spatial neglect and improve function? Frontiers in Rehabilitation Sciences, 6, 1539887. https://doi.org/10.3389/fresc.2025.1539887
- Chen, P., Landar, V., Noce, N., & Hreha, K. (2020). Prism adaptation treatment for spatial neglect post brain tumor removal: A case report. Hong Kong Journal of Occupational Therapy. doi:10.1177/1569186120921472
- Fortis, P., Ronchi, R., Velardo, V., Calzolari, E., Banco, E., Algeri, L., . . . Vallar, G. (2020). A home-based prism adaptation training for neglect patients. Cortex, 122, 61-80. doi:10.1016/j.cortex.2018.09.001
- Goedert, K. M., Chen, P., Foundas, A. L., & Barrett, A. M. (2020). Frontal lesions predict response to prism adaptation treatment in spatial neglect: A randomised controlled study. Neuropsychological Rehabilitation, 30(1), 32-53. doi:10.1080/09602011.2018.1448287
- Chen, P., Goedert, K. M., Shah, P., Foundas, A. L., & Barrett, A. M. (2014). Integrity of medial temporal structures may predict better improvement of spatial neglect with prism adaptation treatment. Brain Imaging and Behavior, 8(3), 346-358. doi:10.1007/s11682-012-9200-5
- Goedert, K. M., Chen, P., Boston, R. C., Foundas, A. L., & Barrett, A. M. (2014). Presence of motor-intentional aiming deficit predicts functional improvement of spatial neglect with prism adaptation. Neurorehabilitation and Neural Repair, 28(5), 483-492.
- Nijboer, T. C., Olthoff, L., Van der Stigchel, S., & Visser-Meily, J. M. (2014). Prism adaptation improves postural imbalance in neglect patients. Neuroreport, 25(5), 307-311. doi:10.1097/WNR.0000000000000088
- Gossmann, A., Kastrup, A., Kerkhoff, G., Lopez-Herrero, C., & Hildebrandt, H. (2013). Prism adaptation improves ego-centered but not allocentric neglect in early rehabilitation patients. Neurorehabilitation and Neural Repair, 27(6), 534-541. doi:10.1177/1545968313478489
- Rabuffetti, M., Folegatti, A., Spinazzola, L., Ricci, R., Ferrarin, M., Berti, A., & Neppi-Modona, M. (2013). Long-lasting amelioration of walking trajectory in neglect after prismatic adaptation. Frontiers in Human Neuroscience, 7, 382. doi:10.3389/fnhum.2013.00382
- Fortis, P., Chen, P., Goedert, K. M., & Barrett, A. M. (2011). Effects of prism adaptation on motor-intentional spatial bias in neglect. Neuroreport, 22(14), 700-705. doi:10.1097/WNR.0b013e32834a3e20
- Mizuno, K., Tsuji, T., Takebayashi, T., Fujiwara, T., Hase, K., & Liu, M. (2011). Prism adaptation therapy enhances rehabilitation of stroke patients with unilateral spatial neglect: A randomized, controlled trial. Neurorehabilitation and Neural Repair, 25(8), 711-720. doi:10.1177/1545968311407516
- Fortis, P., Maravita, A., Gallucci, M., Ronchi, R., Grassi, E., Senna, I., . . . Vallar, G. (2010). Rehabilitating patients with left spatial neglect by prism exposure during a visuomotor activity. Neuropsychology, 24(6), 681-697. doi:10.1037/a0019476
- Jacquin-Courtois, S., Rode, G., Pisella, L., Boisson, D., & Rossetti, Y. (2008). Wheel-chair driving improvement following visuo-manual prism adaptation. Cortex, 44(1), 90-96. doi:10.1016/j.cortex.2006.06.003
- Luaute, J., Michel, C., Rode, G., Pisella, L., Jacquin-Courtois, S., Costes, N., . . . Rossetti, Y. (2006). Functional anatomy of the therapeutic effects of prism adaptation on left neglect. Neurology, 66(12), 1859-1867. doi:10.1212/01.wnl.0000219614.33171.01
- Angeli, V., Benassi, M. G., & Ladavas, E. (2004). Recovery of oculo-motor bias in neglect patients after prism adaptation. Neuropsychologia, 42(9), 1223-1234. doi:10.1016/j.neuropsychologia.2004.01.007
- Farne, A., Rossetti, Y., Toniolo, S., & Ladavas, E. (2002). Ameliorating neglect with prism adaptation: Visuo-manual and visuo-verbal measures. Neuropsychologia, 40(7), 718-729. doi:10.1016/s0028-3932(01)00186-5
- Frassinetti, F., Angeli, V., Meneghello, F., Avanzi, S., & Ladavas, E. (2002). Long-lasting amelioration of visuospatial neglect by prism adaptation. Brain, 125(Pt 3), 608-623. doi:10.1093/brain/awf056
- Rode, G., Rossetti, Y., & Boisson, D. (2001). Prism adaptation improves representational neglect. Neuropsychologia, 39(11), 1250-1254. doi:10.1016/s0028-3932(01)00064-1
- Tilikete, C., Rode, G., Rossetti, Y., Pichon, J., Li, L., & Boisson, D. (2001). Prism adaptation to rightward optical deviation improves postural imbalance in left-hemiparetic patients. Current Biology, 11(7), 524-528. doi:10.1016/s0960-9822(01)00151-8
- Rossetti, Y., Rode, G., Pisella, L., Farne, A., Li, L., Boisson, D., & Perenin, M. T. (1998). Prism adaptation to a rightward optical deviation rehabilitates left hemispatial neglect. Nature, 395(6698), 166-169. doi:10.1038/25988